Introduction | Class 11 Biology Chapter 15 Body Fluids and Circulation notes
Hello students! Welcome back to our journey through human physiology. Today, we are going to talk about the body’s ultimate delivery and waste removal system.
Think about the city or town you live in. What happens if the transport system shuts down? Grocery stores run out of food, garbage piles up on the streets, and everything grinds to a halt. Your body is a bustling metropolis made up of trillions of tiny citizens called cells. These cells constantly need a fresh supply of oxygen, glucose, and nutrients to survive and do their jobs. At the same time, they are constantly generating waste products like carbon dioxide and toxins that need to be cleared out immediately.
How does this exchange happen? Simple organisms like sponges or jellyfish just use the surrounding water. They circulate the ocean water right through their bodies. But you and I are complex beings. We have billions of cells buried deep inside tissues, far away from the outside environment. We cannot rely on surrounding water. Instead, we have evolved a highly sophisticated, closed plumbing system filled with specialized fluids. The main fluid, as you already know, is blood. Another important but often ignored fluid is lymph. In this chapter, we will open the hood of the human body and look at the magnificent pump (the heart), the pipes (blood vessels), and the fluids (blood and lymph) that keep you alive every single second. Let’s dive in!
1. The River of Life: Blood and Its Components
If I ask you what blood is, you might say “it’s a red liquid.” But biologically, blood is classified as a connective tissue. Why a tissue? Because it contains cells. Why connective? Because it connects every single part of your body. Let’s break this incredible fluid down into its two main components: the liquid part (Plasma) and the solid part (Formed Elements).
1.1 Plasma: The Liquid Matrix
Imagine a bowl of soup. The broth is the plasma, and the vegetables are the cells. Plasma makes up about 55% of your total blood volume. It is a slightly yellowish (straw-colored), thick fluid. If we look closely at plasma, it is mostly water (about 90-92%). But floating in this water are extremely important proteins (making up 6-8%).
There are three major proteins you must remember for your exams:
- Fibrinogen: These are the emergency repair workers. Whenever you get a cut, these proteins form a net to clot the blood and stop the bleeding.
- Globulins: Think of these as the defense mechanism of your body. They are primarily antibodies that fight off viruses and bacteria.
- Albumins: These maintain osmotic balance. Simply put, they make sure the water stays inside your blood vessels and doesn’t leak out into your tissues to cause swelling.
Besides proteins, plasma carries a tiny amount of minerals (calcium, magnesium, sodium), glucose, amino acids, and lipids that are in transit to various organs. Teacher’s Note: If you take plasma and remove all the clotting proteins from it, the clear yellow fluid left behind is called Serum.
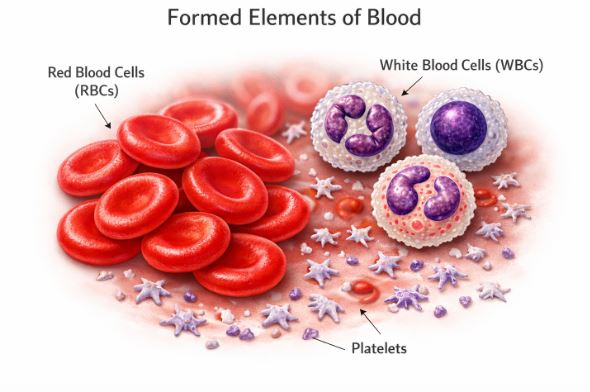
1.2 Formed Elements: The Blood Cells
The remaining 45% of your blood consists of the actual cells, collectively known as formed elements.
A. Erythrocytes (Red Blood Cells or RBCs)
These are the oxygen delivery trucks of your body. They are the most abundant cells, numbering around 5 to 5.5 million per cubic millimeter of blood in a healthy adult man. Where are they born? In the red bone marrow.
Now, here is a fascinating fact: When mature, human RBCs actually kick out their nucleus and other organelles! Why would a cell do that? To make maximum room for a red, iron-containing protein called Haemoglobin. Haemoglobin is what grabs onto oxygen in your lungs. By getting rid of the nucleus, the RBC becomes a biconcave disc (like a donut without the hole punched all the way through), giving it a large surface area to carry as much oxygen as possible.
A healthy person has about 12-16 grams of haemoglobin in every 100 ml of blood. These hardworking cells live for about 120 days. Once they get old and fragile, they are sent to an organ called the spleen to be destroyed. That is why the spleen is often called the “graveyard of RBCs.”
B. Leucocytes (White Blood Cells or WBCs)
If RBCs are the delivery trucks, WBCs are the military and police force. They are colorless because they don’t have haemoglobin, and unlike RBCs, they keep their nucleus. They are much fewer in number (averaging 6000-8000 per cubic millimeter) and are generally short-lived. We divide the WBC army into two main divisions based on whether their cytoplasm looks grainy under a microscope:
- Granulocytes:
- Neutrophils: The most abundant WBCs (60-65%). They are the first responders. They are phagocytic, meaning they literally eat and destroy foreign bacteria.
- Eosinophils: (2-3%). These resist infections and are highly active during allergic reactions.
- Basophils: The rarest (0.5-1%). They secrete chemicals like histamine, serotonin, and heparin, triggering inflammation when you get an infection.
- Agranulocytes:
- Monocytes: (6-8%). Like neutrophils, these are big phagocytic cells that eat invading organisms.
- Lymphocytes: (20-25%). The masterminds of your immune system. They come in two major types: B-lymphocytes and T-lymphocytes. They are responsible for your body’s specific immune responses and creating antibodies.
C. Platelets (Thrombocytes)
These are not full cells; they are actually broken-off cell fragments produced by giant cells in the bone marrow called megakaryocytes. You have about 1.5 to 3.5 lakh platelets per cubic millimeter of blood. Their only job is to rush to the site of an injury and release substances that cause your blood to clot, preventing you from bleeding to death.
2. Blood Groups: Why We Cannot Mix All Blood
Have you ever wondered why a hospital asks for a specific blood type before surgery? Even though all human blood looks red and identical, the surface of our Red Blood Cells carries distinct chemical name tags. These name tags are called antigens. If you put the wrong blood into someone’s body, their immune system will attack these unfamiliar antigens, causing the blood to clump together (agglutination) and destroy the RBCs. This is fatal.
2.1 ABO Grouping
The ABO system is based on the presence or absence of two specific surface antigens on the RBCs: Antigen A and Antigen B. At the same time, your plasma naturally contains antibodies against the antigens you DO NOT have. Let’s make it simple:
- If you have Blood Group A, your RBCs have Antigen A. Your plasma has “anti-B” antibodies. (You can receive A or O blood).
- If you have Blood Group B, your RBCs have Antigen B. Your plasma has “anti-A” antibodies. (You can receive B or O blood).
- If you have Blood Group AB, you have both A and B antigens! Because you have both, your body doesn’t produce any antibodies against them. This makes you a Universal Recipient. You can accept blood from anyone.
- If you have Blood Group O, your RBCs have NO antigens on the surface. They are like blank slates. Because they are blank, they won’t trigger an attack in anyone else’s body. This makes O group individuals Universal Donors. However, because they have no antigens, their plasma contains both anti-A and anti-B antibodies. They can only receive O blood.
2.2 The Rh Factor and Pregnancy Complications
There is another antigen called the Rh factor, first discovered in Rhesus monkeys. About 80% of humans have this antigen on their RBCs, making them Rh positive (Rh+ve). The other 20% lack it and are Rh negative (Rh-ve).
This becomes extremely critical during pregnancy in a specific scenario: an Rh-ve mother carrying an Rh+ve baby. During the first pregnancy, the mother’s and baby’s blood do not mix because of the placenta. However, during delivery, some of the baby’s Rh+ve blood might leak into the mother’s bloodstream. The mother’s immune system sees this Rh antigen as an alien invader and starts building “anti-Rh” antibodies.
If the mother gets pregnant again with a second Rh+ve baby, her previously made anti-Rh antibodies will cross the placenta, attack the baby’s RBCs, and destroy them. This severe, potentially fatal condition for the foetus is called Erythroblastosis foetalis, leading to severe anaemia and jaundice in the baby. How do we prevent this? Doctors simply administer special anti-Rh antibodies to the mother immediately after her first delivery to neutralize any leaked foetal blood cells before her immune system can react.
3. Coagulation of Blood: The Body’s Sealant
When you cut your finger while chopping vegetables, it bleeds for a minute and then automatically stops. A dark reddish-brown scab forms. How does a liquid suddenly turn into a solid plug? This is the magic of blood coagulation.
It is a brilliant, domino-like chain reaction (a cascade process) involving enzymes and calcium ions. Here is how the sequence flows:
- The Alarm: An injury stimulates your platelets and damaged tissues to release certain chemical factors.
- The Catalyst: These factors trigger the formation of an enzyme complex called Thrombokinase.
- The Activation: In your plasma, there is a sleeping, inactive protein called Prothrombin. Thrombokinase wakes it up and converts it into an active enzyme called Thrombin.
- The Net: Thrombin then takes another dissolved protein called Fibrinogen and converts it into solid, insoluble threads called Fibrin.
These fibrin threads form a sticky mesh at the wound site, trapping dead and damaged blood cells. This block is what we call a clot or coagulum. Teacher’s Hint: Never forget that Calcium ions ($Ca^{++}$) are absolutely essential for these clotting reactions to occur!
4. Lymph: The Middleman of the Body
Blood flows inside closed tubes (capillaries). But cells are sitting outside these tubes. So how does a glucose molecule move from the blood into a muscle cell?
As blood flows under high pressure through tiny, thin-walled capillaries, some water, nutrients, and small water-soluble substances are squeezed out through the capillary walls into the empty spaces between your tissue cells. This fluid bathing your cells is called Interstitial Fluid or Tissue Fluid. It leaves behind the large proteins and RBCs inside the blood vessel.
This tissue fluid is the actual medium where the exchange of oxygen, nutrients, and waste happens. Once the exchange is done, this fluid cannot just stay there, or you would swell up like a balloon. It is collected by an entirely separate, one-way drainage system called the Lymphatic System. Once this tissue fluid enters the lymphatic vessels, we call it Lymph.
Lymph is a colorless fluid. It contains specialized lymphocytes for immune responses. Importantly, lymph is also responsible for absorbing digested fats from your intestine through specialized vessels called lacteals located in the intestinal villi. Ultimately, the lymphatic vessels carry this fluid and dump it back into your major veins near the heart.
5. The Engine Room: Human Circulatory System
Now we arrive at the most vital organ of this entire transport system: The Heart.
5.1 Evolutionary Background
Before we look at humans, let’s see how the heart evolved in vertebrates. Fishes have a simple 2-chambered heart (one atrium, one ventricle) that pumps deoxygenated blood to the gills, which then goes to the body and back to the heart. This is single circulation. Amphibians and reptiles (except crocodiles) upgraded to a 3-chambered heart (two atria, one ventricle). They receive oxygenated and deoxygenated blood separately in the atria, but it mixes in the single ventricle. Birds and mammals, including humans, possess a highly efficient 4-chambered heart. The left and right sides are completely separated, ensuring oxygen-rich and oxygen-poor blood never mix. This is why we have Double Circulation.
5.2 Structure of the Human Heart
Your heart is derived from the mesoderm embryonic layer. It sits in your thoracic cavity between the two lungs, slightly tilted to the left, and is about the size of your clenched fist. To protect it from friction as it beats, it is wrapped in a double-layered membrane bag called the Pericardium, filled with lubricating pericardial fluid.
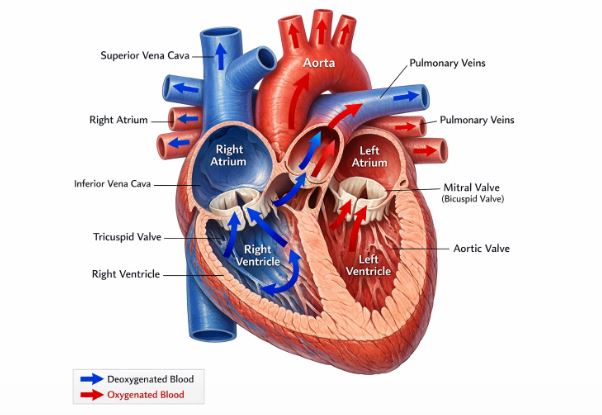
The heart has four rooms: two smaller upper rooms called Atria (receiving chambers) and two larger, highly muscular lower rooms called Ventricles (pumping chambers).
To keep blood flowing in exactly one direction, the heart has doors called valves:
- Tricuspid Valve: Located between the Right Atrium and Right Ventricle. It has three muscular flaps.
- Bicuspid (or Mitral) Valve: Located between the Left Atrium and Left Ventricle. It has two flaps.
- Semilunar Valves: Located at the exit doors of the ventricles, guarding the opening to the pulmonary artery and the aorta.
The muscular walls of the ventricles are much thicker than the atria because they have to pump blood over long distances. The left ventricle is the thickest of all because it pumps blood to the entire body against high pressure.
5.3 The Pacemaker: Nodal Tissue
Your heart doesn’t need your brain to tell it to beat! It is auto-excitable. The heart wall has patches of specialized muscle fibers that generate electrical signals. The most important one is the Sino-Atrial Node (SAN), located in the upper right corner of the right atrium. It acts as the natural pacemaker, generating 70-75 electrical impulses per minute, setting the rhythm of your heartbeat.
The signal travels from the SAN to the Atrio-Ventricular Node (AVN), down through the Bundle of His, and spreads into the ventricular walls via Purkinje fibres, causing the muscles to contract in a beautifully coordinated wave.
6. The Cardiac Cycle and ECG
The sequence of events in one complete heartbeat is called the Cardiac Cycle. It lasts for just 0.8 seconds! It consists of alternating phases of contraction (Systole) and relaxation (Diastole).
Let’s walk through one cycle:
- Joint Diastole: All four chambers are relaxed. Blood flows from veins passively into the atria and down into the ventricles through the open bicuspid/tricuspid valves.
- Atrial Systole: The SAN fires! Both atria contract together, squeezing the remaining 30% of blood down into the ventricles.
- Ventricular Systole: The ventricles contract powerfully. Pressure builds up instantly. The blood tries to rush back up into the atria, which slams the tricuspid and bicuspid valves shut. (This produces the first heart sound: LUB). The high pressure forces open the semilunar valves, and blood shoots out into the aorta and pulmonary artery.
- Ventricular Diastole: The ventricles relax. The pressure drops. To prevent blood from falling back from the aorta into the heart, the semilunar valves snap shut. (This produces the second heart sound: DUB).
Cardiac Output: In one beat, a ventricle pumps out about 70 mL of blood (Stroke Volume). Multiply that by your heart rate (72 beats/min), and you get the Cardiac Output: roughly 5000 mL or 5 Litres of blood pumped every single minute!
Understanding the ECG
When a patient is hooked to an electrocardiograph machine, the graphical readout on the paper is the Electrocardiogram (ECG). It maps the electrical journey of a heartbeat.
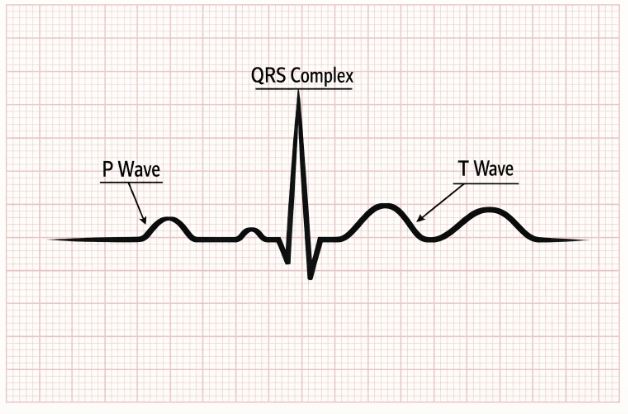
- P-Wave: Represents the electrical excitation (depolarisation) of the atria right before they contract.
- QRS Complex: Represents the depolarisation of the ventricles. This marks the powerful ventricular contraction.
- T-Wave: Represents the return of the ventricles to a normal, relaxed state (repolarisation).
By counting the QRS complexes, doctors can instantly calculate your heart rate. Any change in the shape of these waves indicates heart damage or disease.
7. Double Circulation and Regulation
We have two separate pathways working simultaneously, creating a figure-eight loop:
- Pulmonary Circulation: The Right Ventricle pumps dark, deoxygenated blood to the lungs via the pulmonary artery. It gets oxygenated in the lungs and returns bright red to the Left Atrium via pulmonary veins.
- Systemic Circulation: The Left Ventricle pumps the oxygenated blood through the aorta to the entire body, delivering nutrients. The depleted, deoxygenated blood is gathered by the vena cava and returned to the Right Atrium.
Regulation: Though the heart is myogenic (sets its own beat), your brain can moderate it. A center in the medulla oblongata uses the Autonomic Nervous System (ANS). Sympathetic nerves release signals that increase heart rate and pumping strength (like when you are running or scared). Parasympathetic nerves decrease the heart rate, returning you to a resting state.
8. Disorders of the Circulatory System
Like any mechanical pump and pipe system, things can go wrong over time.
- High Blood Pressure (Hypertension): Normal BP is 120/80 (Systolic/Diastolic). If it consistently stays above 140/90, the person has hypertension. It forces the heart to work harder and damages blood vessels, the brain, and kidneys.
- Coronary Artery Disease (CAD): Also known as atherosclerosis. This is when calcium, fat, and cholesterol build up as plaque inside the arteries supplying the heart muscle itself, making the tubes narrow.
- Angina (Angina Pectoris): A severe, acute chest pain that happens when the heart muscle isn’t getting enough oxygen, usually due to narrowed blood vessels.
- Heart Failure: The heart becomes weak and cannot pump blood effectively enough to meet the body’s demands. It often leads to lung congestion. Note: This is different from a heart attack, where the heart muscle actually dies due to a blocked blood supply.
Real-Life Examples to Understand Circulation
- The Highway System: Think of the heart as the main central station. The arteries are the massive outgoing highways moving traffic away at high speeds. Capillaries are the tiny, narrow local street alleys where deliveries (oxygen/nutrients) are made to individual houses (cells). The veins are the slow return roads bringing empty trucks back to the station.
- Plumbing Leaks and Platelets: If a pipe bursts in your house, you call a plumber to patch the hole with cement. When a blood vessel tears, platelets act as microscopic plumbers, immediately rushing to the site and laying down a cement net (fibrin) to seal the leak.
Key Takeaways & Summary
- Blood is a fluid connective tissue made of plasma (55%) and formed elements (45%).
- RBCs transport respiratory gases. WBCs fight infections. Platelets help in coagulation.
- Blood groups (ABO and Rh) must be carefully matched before a transfusion to prevent fatal clumping. ‘O’ is universal donor; ‘AB’ is universal recipient.
- Tissue fluid (Lymph) acts as a middleman for exchange and drains back into the venous system.
- Humans possess a closed double circulatory system with a 4-chambered myogenic heart.
- The Cardiac cycle involves systole (contraction) and diastole (relaxation), producing ‘lub’ and ‘dub’ sounds, and is graphically represented by an ECG.
Common Student Misconceptions
Misconception 1: Arteries always carry oxygenated blood and veins always carry deoxygenated blood.
Correction: While mostly true, there is a major exception! The Pulmonary Artery carries deoxygenated blood from the heart to the lungs. The Pulmonary Vein carries oxygenated blood from the lungs to the heart. The real definition is: Arteries carry blood AWAY from the heart, and veins bring blood TOWARDS the heart.
Misconception 2: Cardiac arrest, heart attack, and heart failure are all the exact same thing.
Correction: They are distinct conditions. Heart failure is when the heart is weak and pumping poorly. A heart attack is a plumbing problem; a blood vessel gets blocked, and a portion of the heart muscle starves and dies. Cardiac arrest is an electrical problem; the heart’s pacemaker malfunctions, and the heart suddenly stops beating completely.
Practice Set: Test Your Knowledge (CBSE Pattern)
Very Short Answer Questions (1-2 Marks)
Q1. Why is the sino-atrial node (SAN) called the pacemaker of our heart?
Answer: The SAN is called the pacemaker because it generates the maximum number of electrical action potentials (70-75 per minute). It initiates and maintains the rhythmic contractile activity of the entire heart.
Q2. Name the fluid that leaves the capillaries and bathes the tissue cells. State one major function of it.
Answer: The fluid is called interstitial fluid or tissue fluid (which becomes lymph when it enters lymphatic vessels). Its major function is to act as the medium for the exchange of nutrients, oxygen, and waste products between the blood and the tissue cells.
Q3. What do the ‘lub’ and ‘dub’ sounds of the heart signify?
Answer: The ‘lub’ (first sound) signifies the closure of the tricuspid and bicuspid (AV) valves during ventricular contraction. The ‘dub’ (second sound) signifies the closure of the semilunar valves during ventricular relaxation.
Short Answer Questions (3 Marks)
Q4. Explain the difference between blood and lymph.
Answer:
1. Composition: Blood contains RBCs, WBCs, platelets, and plasma with a high protein concentration. Lymph is a colorless fluid lacking RBCs, having fewer platelets, and a lower protein concentration; it is rich in specialized lymphocytes.
2. Flow: Blood flows rapidly in a circular, closed loop pumped by the heart. Lymph flows slowly in a one-way direction from tissues towards the heart.
3. Function: Blood transports oxygen, nutrients, and waste. Lymph primarily helps in immune responses, returns leaked fluid to the blood, and absorbs fats from the intestines.
Q5. Briefly describe the cascade process of blood coagulation.
Answer: When an injury occurs, platelets and damaged tissues release factors that form an enzyme complex called thrombokinase. Thrombokinase converts the inactive plasma protein prothrombin into the active enzyme thrombin. Thrombin then acts as a catalyst to convert soluble fibrinogen into insoluble fibrin threads. These threads form a mesh that traps dead and damaged blood cells, creating a clot. Calcium ions are essential for this entire pathway.
Long Answer Questions (5 Marks)
Q6. Define a cardiac cycle. Describe the major events occurring during a single cardiac cycle.
Answer: The cyclic, sequential repetition of events in the heart for a single heartbeat is called the cardiac cycle, lasting 0.8 seconds. It involves:
1. Joint Diastole: All four chambers are relaxed. Blood from major veins fills the right and left atria and flows passively into the ventricles through open AV valves.
2. Atrial Systole: The SAN fires an action potential, causing both atria to contract simultaneously. This pushes the remaining 30% of blood into the ventricles.
3. Ventricular Systole: The action potential reaches the ventricles via the AVN and bundle of His. Ventricles contract, raising pressure. This forces the AV valves to shut (lub sound) to prevent backflow, and forces the semilunar valves open, pumping blood into the aorta and pulmonary artery.
4. Ventricular Diastole: Ventricles relax, dropping pressure. Semilunar valves snap shut (dub sound) to prevent backward flow from the arteries. The AV valves open again, and the cycle repeats.
Q7. Draw a standard ECG and explain its different segments. Why is it clinically significant?
Answer: (Students should practice drawing the P-QRS-T wave diagram as shown in the textbook).
– P-wave: Represents the electrical excitation or depolarisation of the atria, leading to atrial systole (contraction).
– QRS complex: Represents the depolarisation of the ventricles, which triggers ventricular systole. The contraction starts shortly after the Q wave.
– T-wave: Represents repolarisation, where the ventricles return to their normal relaxed state. The end of the T-wave marks the end of ventricular systole.
Clinical significance: Because a normal ECG has a very specific, standard shape, any deviation in the peaks or intervals can help doctors easily identify heart diseases, abnormal rhythms, or a damaged heart muscle.
Case-Based / Competency-Based Question (4 Marks)
Q8. Read the clinical scenario and answer the questions.
A 28-year-old pregnant woman visits her gynaecologist for a routine check-up during her second pregnancy. Her blood report shows her blood group is B Negative (Rh-ve). She mentions that her first child was born healthy, and the child’s blood group is B Positive (Rh+ve). The doctor immediately asks if she was given a specific injection right after her first delivery.
(a) Which specific injection is the doctor asking about?
(b) Why is this medical history critical for her current second pregnancy?
(c) Name the medical condition that could affect the foetus if this precaution was ignored.
Answer:
(a) The doctor is asking if she received an injection of anti-Rh antibodies immediately after the delivery of her first child.
(b) During her first delivery of an Rh+ve baby, some foetal blood likely mixed with her Rh-ve blood. This causes her immune system to produce destructive anti-Rh antibodies. If the current foetus is also Rh+ve, these maternal antibodies can cross the placenta and destroy the foetus’s red blood cells.
(c) The condition is called Erythroblastosis foetalis, which causes severe anaemia and jaundice, and can be fatal to the baby.
Assertion-Reason Question
Q9. For the following question, two statements are given—one labeled Assertion (A) and the other labeled Reason (R). Select the correct answer from the codes (a), (b), (c), and (d) as given below.
(a) Both A and R are true, and R is the correct explanation of A.
(b) Both A and R are true, but R is not the correct explanation of A.
(c) A is true, but R is false.
(d) A is false, but R is true.
Assertion (A): A person with blood group AB is considered a universal recipient.
Reason (R): The plasma of a person with blood group AB contains both anti-A and anti-B antibodies.
Answer: (c) A is true, but R is false.
Explanation: The assertion is correct; AB individuals can receive blood from any group. However, the reason is false. An AB individual has both A and B antigens on their RBCs, which is exactly why they have NO antibodies (neither anti-A nor anti-B) in their plasma. If they had those antibodies, they would attack the incoming blood.
End of Notes.
Students, make sure you understand the sequence of the cardiac cycle, the flow of double circulation, and the cascade of blood clotting. Practice drawing the human heart and the ECG graph. Keep revising, and happy learning!
Read Also:
Chapter 14- Breathing and Exchange of Gases
For official syllabus and textbooks, visit the
NCERT Official Website.