Introduction | Breathing vs. Respiration
Hello students! Welcome back to another exciting journey into Human Physiology. Today, we are going to talk about something you are doing right at this very second without even thinking about it: breathing. But have you ever paused to ask yourself, why exactly do we breathe?
Up until now, you might have used the words “breathing” and “respiration” interchangeably. However, in biology, we need to be very precise. Our bodies are made of trillions of cells, and every single one of those cells is like a tiny factory working around the clock. To do their jobs—whether it’s muscle contraction, sending nerve impulses, or digesting food—they need energy. They get this energy by breaking down nutrient molecules, like glucose, amino acids, and fatty acids.
But here is the catch: to break down these molecules efficiently and extract maximum energy, the cells desperately need oxygen ($O_2$). As a byproduct of this energy production, the cells create carbon dioxide ($CO_2$), which is essentially toxic waste for our body. This means we need a reliable delivery system to continuously supply fresh oxygen to the cells and a robust garbage disposal system to throw the carbon dioxide out.
The physical act of drawing in fresh atmospheric air and expelling stale, $CO_2$-rich air is what we call breathing. The actual cellular utilization of that oxygen to produce energy is cellular respiration. In this chapter, we will focus on the fascinating machinery that makes the physical exchange of these gases possible. Let’s dive in!
1. The Evolution of Respiratory Organs
1.1 How Different Animals Breathe
Nature is incredibly resourceful. Depending on where an animal lives (its habitat) and how complex its body is, the mechanism of breathing varies widely.
- Simple Diffusion: Lower invertebrates like sponges, flatworms, and coelenterates don’t have lungs or gills. They simply allow oxygen to diffuse into their bodies and carbon dioxide to diffuse out across their entire body surface.
- Cutaneous Respiration: Have you ever seen a shiny, moist earthworm? They use their wet skin (cuticle) to exchange gases. Even frogs can breathe through their moist skin when they are in water.
- Tracheal Tubes: Insects have an intricate network of tiny tubes running throughout their bodies that carry atmospheric air directly to their tissues.
- Branchial Respiration (Gills): For creatures living underwater, like fish and many aquatic arthropods and molluscs, special highly vascularized structures called gills are the organs of choice.
- Pulmonary Respiration (Lungs): For terrestrial vertebrates—like reptiles, birds, and us mammals—we use vascularized bags called lungs to exchange gases.
1.2 The Human Respiratory System: A Guided Tour
Let’s trace the journey of a breath of air as it enters your body. We start at the external nostrils, which open just above your upper lip. When you inhale, air passes through the nasal passage into the nasal chamber.
From there, the air moves into the pharynx. Think of the pharynx as a busy intersection; it is the common passageway for both the air you breathe and the food you eat. But we don’t want food going into our lungs, right? That’s where a brilliant little flap called the epiglottis comes in. Made of elastic cartilage, it acts like a trapdoor, covering the windpipe opening (glottis) when you swallow so food goes down the right pipe.
The air then passes through the larynx, a cartilaginous box famously known as the sound box because it houses our vocal cords. Next, it travels down the trachea (windpipe). The trachea is a straight tube that goes down to your mid-chest cavity, where it splits into two paths: the right and left primary bronchi (this split happens around the level of the 5th thoracic vertebra).
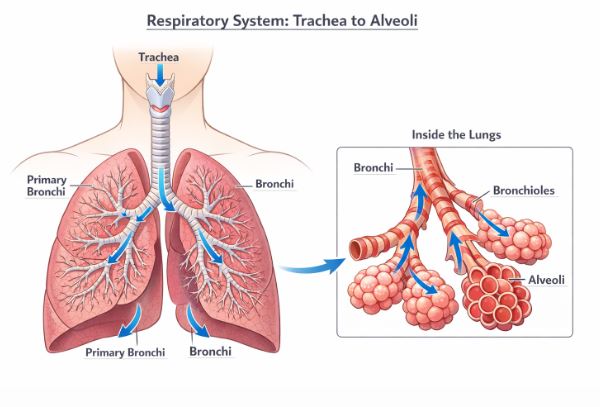
Once inside the lungs, each primary bronchus divides into secondary bronchi, then tertiary bronchi, and finally into tiny tubes called bronchioles. To keep these vital airways from collapsing under pressure, the trachea and the bronchi are supported by incomplete rings of cartilage.
At the very end of the terminal bronchioles, we find the real stars of the show: the alveoli. These are very thin, irregularly shaped, highly vascularized (meaning they have lots of blood vessels) bag-like structures.
Teacher’s Tip: The Respiratory System has Two Main Parts!
- The Conducting Part: Everything from the nostrils down to the terminal bronchioles. This part doesn’t exchange gases. Its job is to transport the air, filter out dust and foreign particles, add moisture (humidify), and warm the air to match your body temperature.
- The Exchange Part: The alveoli and their associated ducts. This is where the actual magic of gas diffusion happens between the air and your blood.
Our two lungs are safely enclosed in a double-layered membrane called the pleura. Between these two layers is the pleural fluid, which acts like engine oil to reduce friction when your lungs expand and rub against the chest wall. The lungs are housed in the thoracic chamber, an air-tight vault protected by your backbone (dorsally), the breastbone/sternum (ventrally), the ribs (laterally), and a muscular dome called the diaphragm at the bottom.
2. The Mechanism of Breathing
How do we actually pull air in and push it out? It all comes down to basic physics: Pressure!
Breathing happens in two distinct stages: Inspiration (drawing air in) and Expiration (pushing alveolar air out). We do not have muscles directly attached to the lungs to pull them open. Instead, we alter the volume of our chest cavity.
Air always flows from an area of high pressure to an area of low pressure. To draw air into our lungs, the pressure inside our lungs (intra-pulmonary pressure) must be lower than the pressure of the atmosphere outside. Conversely, to push air out, the pressure inside must be higher than the atmospheric pressure.
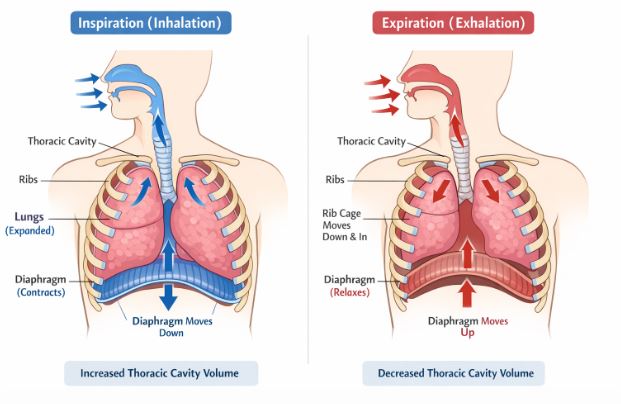
2.1 Inspiration (Breathing In)
When you decide to take a breath, the primary breathing muscle, the diaphragm, contracts. When it contracts, it flattens and moves downward, increasing the length of the chest cavity from top to bottom (antero-posterior axis).
Simultaneously, a specialized set of muscles located between your ribs, called the external intercostal muscles, contract. This action pulls your ribs and sternum upwards and outwards, increasing the chest volume from front to back (dorso-ventral axis).
Because the lungs are perfectly stuck to the inside of the chest wall (thanks to the pleural membranes), an increase in the chest cavity volume forces the lungs to expand. Greater volume means lower pressure. Now, the intra-pulmonary pressure drops below atmospheric pressure, and air rushes in from the outside to fill the vacuum.
2.2 Expiration (Breathing Out)
Normal expiration is largely a passive process. The diaphragm and the external intercostal muscles simply relax. The diaphragm returns to its original dome shape, and the ribs fall back to their resting position. This reduces the volume of the chest cavity, which in turn reduces the volume of the lungs. With the volume decreased, the pressure inside the lungs briefly spikes above atmospheric pressure, forcing the air out.
Fun Fact: While normal breathing uses these basic muscles, if you are blowing up a tough balloon or exercising hard, you can forcefully exhale by recruiting additional muscles in your abdomen! An average, healthy adult takes about 12 to 16 breaths every single minute.
3. Respiratory Volumes and Capacities
Just like a bank tracks how much money goes in and out of your account, doctors use a machine called a spirometer to measure the volume of air moving in and out of your lungs. This helps them check if your lungs are functioning healthily. Let’s look at the “currency” of respiration.
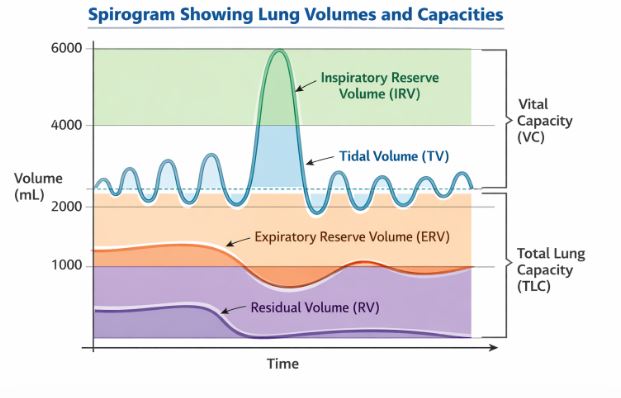
3.1 Primary Lung Volumes
- Tidal Volume (TV): Think of this as your regular, daily pocket money. It is the amount of air you breathe in or out during normal, relaxed breathing. For a healthy adult, it is about 500 mL per breath. Over a minute, that equals roughly 6000 to 8000 mL of air!
- Inspiratory Reserve Volume (IRV): This is your emergency borrowing power. After a normal breath in, if you take a deep, forceful gasp to fill your lungs to the absolute maximum, the extra air you pull in is the IRV. It averages around 2500 mL to 3000 mL.
- Expiratory Reserve Volume (ERV): This is forcefully spending your savings. After a normal breath out, the extra volume of air you can forcefully push out of your lungs is the ERV. It averages about 1000 mL to 1100 mL.
- Residual Volume (RV): This is the minimum balance required to keep the bank account open. Even if you push out as much air as you physically can, your lungs never completely empty. The volume of air that always remains trapped in the lungs is the RV. It averages 1100 mL to 1200 mL. This prevents your delicate alveoli from collapsing!
3.2 Pulmonary Capacities (Combining Volumes)
By adding these specific volumes together, doctors can calculate your lung capacities:
- Inspiratory Capacity (IC): Total air you can breathe in after a normal breath out. Formula: TV + IRV.
- Expiratory Capacity (EC): Total air you can push out after a normal breath in. Formula: TV + ERV.
- Functional Residual Capacity (FRC): The total air left in your lungs after a normal, relaxed exhalation. Formula: ERV + RV.
- Vital Capacity (VC): The absolute maximum amount of air you can cycle through your lungs. It’s the maximum you can exhale after a maximum inhalation. Formula: ERV + TV + IRV.
- Total Lung Capacity (TLC): The total volume of air your lungs can hold at maximum inflation. Formula: RV + ERV + TV + IRV (or simply Vital Capacity + Residual Volume).
4. The Exchange of Gases
So, the fresh air has reached the alveoli. What happens next? A critical exchange takes place via simple diffusion. Oxygen moves from the alveoli into the blood, and carbon dioxide moves from the blood into the alveoli. Later, a similar exchange happens between the blood and your body tissues.
4.1 Understanding Partial Pressure
To understand diffusion, you must understand Partial Pressure. Air is a mixture of gases (nitrogen, oxygen, carbon dioxide, etc.). The pressure exerted by one specific gas in this mixture is its partial pressure. We write it as $pO_2$ for oxygen and $pCO_2$ for carbon dioxide. Gases are like water; they always flow downhill from a region of higher partial pressure to a region of lower partial pressure.
Let’s look at the numbers. In the alveoli, the $pO_2$ is a high 104 mm Hg. The deoxygenated blood arriving at the lungs has a $pO_2$ of only 40 mm Hg. Because 104 is much higher than 40, oxygen easily diffuses down the gradient from the alveoli into the blood.
Conversely, the $pCO_2$ in the deoxygenated blood is 45 mm Hg, while it is only 40 mm Hg in the alveoli. So, $CO_2$ diffuses out of the blood and into the alveoli to be exhaled.
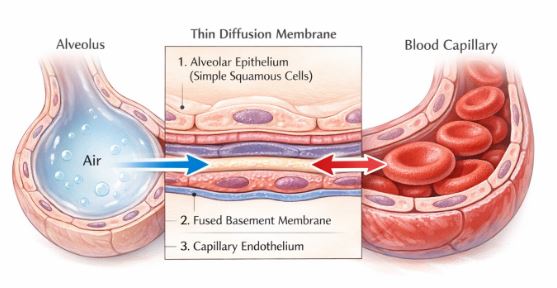
4.2 Factors Affecting the Rate of Diffusion
Two major factors decide how fast and efficiently gases exchange:
- Solubility of the Gas: Carbon dioxide is highly soluble—about 20 to 25 times more soluble than oxygen! Because of this, even a small pressure difference (like 45 to 40 mm Hg) allows a massive amount of $CO_2$ to diffuse rapidly across the membrane.
- Thickness of the Membrane: The thinner the barrier, the faster the diffusion. The diffusion membrane in our lungs is incredibly thin (less than a millimeter thick!). It consists of three extremely delicate layers: the single-celled squamous epithelium of the alveoli, the endothelial lining of the blood capillaries, and a thin basement substance sandwiched between them.
5. Transport of Gases in the Blood
Once gases diffuse into the bloodstream, they need vehicles to transport them throughout the body’s highway system.
5.1 Transport of Oxygen
Oxygen doesn’t dissolve very well in water, which makes up most of blood plasma. Therefore, only about 3% of $O_2$ is carried in a dissolved state in the plasma. The heavy lifting is done by the Red Blood Cells (RBCs), which carry a whopping 97% of the oxygen.
Inside the RBCs is a red, iron-containing protein pigment called Haemoglobin. Haemoglobin acts like a molecular taxi. Oxygen binds to haemoglobin in a reversible manner to form oxyhaemoglobin. A single haemoglobin molecule has four seats, meaning it can carry a maximum of four $O_2$ molecules at a time.
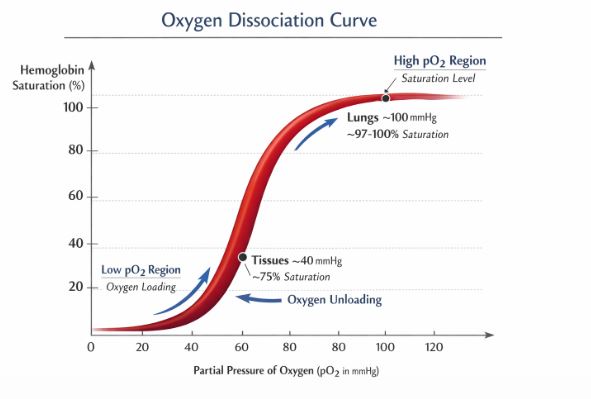
The binding of oxygen depends largely on the partial pressure of oxygen ($pO_2$). If we plot the percentage saturation of haemoglobin against the $pO_2$, we get a highly characteristic S-shaped graph known as the Oxygen Dissociation Curve.
Haemoglobin is very smart. It knows exactly where to pick up passengers and where to drop them off:
- At the Lungs (Pickup Zone): The conditions are perfect for binding—high $pO_2$, low $pCO_2$, low $H^+$ (acid) concentration, and lower temperature. Haemoglobin eagerly grabs oxygen.
- At the Tissues (Drop-off Zone): The tissues are working hard, producing waste. Here, there is low $pO_2$, high $pCO_2$, high $H^+$ concentration, and a higher temperature. These conditions act as a signal, causing haemoglobin to release (dissociate) its oxygen to feed the hungry cells. Under normal conditions, every 100 mL of oxygenated blood delivers about 5 mL of $O_2$ to your tissues.
5.2 Transport of Carbon Dioxide
Carbon dioxide is handled a bit differently. Because it is highly soluble, about 7% travels dissolved directly in the plasma. Another 20-25% hitches a ride on haemoglobin, binding to the protein part to form carbamino-haemoglobin.
However, the vast majority—nearly 70%—is transported in the form of bicarbonate ions ($HCO_3^-$). Inside your RBCs, there is a very powerful enzyme called carbonic anhydrase (a tiny amount is also in the plasma). At the tissues where $CO_2$ is high, this enzyme grabs $CO_2$ and water ($H_2O$) and converts them into carbonic acid ($H_2CO_3$), which quickly breaks down into a bicarbonate ion ($HCO_3^-$) and a hydrogen ion ($H^+$).
This bicarbonate floats safely in the blood to the lungs. Once at the alveolar site where $pCO_2$ is low, the brilliant enzyme runs the reaction in reverse! It turns the bicarbonate back into $CO_2$ and water, allowing the $CO_2$ to diffuse into the lungs and be exhaled. Every 100 mL of deoxygenated blood delivers roughly 4 mL of $CO_2$ to the alveoli.
6. Regulation of Respiration
Have you ever tried to hold your breath? Eventually, an overwhelming urge forces you to gasp for air. This is because your breathing is tightly controlled by your neural system to perfectly match your body’s demands.
The primary pacemaker for your breathing is the respiratory rhythm centre, located in the medulla region of your brain. A backup controller, called the pneumotaxic centre, is located nearby in the pons region of the brain. This centre acts like a brake; it can send signals to reduce the duration of inspiration, thereby increasing your overall breathing rate when you need to breathe faster.
Right next to the rhythm centre is a highly sensitive chemosensitive area. Here is the surprising part: this area does NOT care about oxygen! It is highly sensitive to carbon dioxide ($CO_2$) and Hydrogen ions ($H^+$). If $CO_2$ or acid levels rise in your blood, this centre gets activated and immediately signals the rhythm centre to make you breathe faster and deeper to clear out the toxic waste. Additional sensors in your aortic arch and carotid artery also constantly monitor the blood for high $CO_2$ and $H^+$ levels.
7. Disorders of the Respiratory System
Unfortunately, our delicate respiratory system can fall victim to several disorders.
- Asthma: This is an allergic or inflammatory condition affecting the bronchi and bronchioles. The airways swell and narrow, making it very difficult to breathe and producing a characteristic wheezing sound.
- Emphysema: This is a chronic, devastating disease where the delicate walls of the alveoli are permanently damaged. This drastically reduces the surface area available for gas exchange. The number one major cause of this irreversible condition is cigarette smoking.
- Occupational Respiratory Disorders: In industries like stone breaking, grinding, or mining, massive amounts of fine dust are produced. Your body’s natural defense mechanisms cannot clear it all. Over long periods, the continuous irritation causes severe inflammation leading to fibrosis (proliferation of rigid, fibrous scar tissue in the lungs). This causes permanent lung damage. Workers in such environments must prioritize safety and wear protective masks.
Key Takeaways & Summary
- Respiration begins with breathing (ventilation), followed by the exchange of gases at the alveoli, transport through the blood, exchange at the tissues, and finally cellular respiration.
- The human respiratory system consists of a conducting zone (nostrils to terminal bronchioles) and an exchange zone (alveoli).
- Breathing is driven by pressure gradients created by the diaphragm and intercostal muscles changing the volume of the thoracic cavity.
- Gas exchange is a passive process of simple diffusion, dependent on partial pressure gradients, gas solubility, and membrane thickness.
- 97% of Oxygen is transported bound to haemoglobin in RBCs. 70% of Carbon Dioxide is transported as bicarbonate in the blood.
- The respiratory rhythm is primarily controlled by the medulla and pons in the brain, heavily influenced by $CO_2$ and $H^+$ concentrations, rather than oxygen levels.
Common Student Misconceptions
Misconception 1: “We breathe faster during exercise because our brain detects low oxygen levels.”
Correction: While it seems logical, the respiratory centers in our brain are actually relatively blind to oxygen. We breathe faster primarily because our brain detects the rapid buildup of carbon dioxide and hydrogen ions produced by working muscles. $CO_2$ is the primary driver of breathing!
Misconception 2: “When we exhale completely, our lungs are totally empty.”
Correction: Never! Due to the rigid structure of the rib cage and the pleural fluids, your lungs can never completely collapse. Even after the most forceful expiration, a significant amount of air, called the Residual Volume (approx. 1100-1200 mL), remains trapped inside.
Practice Set: Test Your Knowledge (CBSE Pattern)
Very Short Answer Questions (1 Mark)
Q1. Which important enzyme is present in a high concentration within RBCs that facilitates the transport of carbon dioxide?
Answer: Carbonic anhydrase.
Q2. State the volume of air remaining in the lungs after a normal breathing expiration.
Answer: This is known as the Functional Residual Capacity (FRC). It includes the Expiratory Reserve Volume (ERV) plus the Residual Volume (RV).
Short Answer Questions (2-3 Marks)
Q3. Diffusion of gases occurs in the alveolar region only and not in the other parts of the respiratory system. Why?
Answer: The conducting parts of the respiratory tract (trachea, bronchi) have thick walls supported by cartilaginous rings, which are unsuitable for diffusion. The alveoli, however, have extremely thin, highly vascularized squamous epithelial walls. The total thickness of the diffusion membrane here is less than a millimeter, making it the ideal and only functional site for rapid gas exchange.
Q4. Explain the role of the diaphragm during inspiration under normal conditions.
Answer: Inspiration is initiated by the contraction of the diaphragm. Upon contraction, it moves downward, which increases the overall volume of the thoracic chamber in the antero-posterior axis. This increase in volume leads to a decrease in intra-pulmonary pressure, creating a negative pressure gradient that draws atmospheric air into the lungs.
Long Answer Questions (5 Marks)
Q5. What are the major transport mechanisms for $CO_2$? Explain in detail.
Answer: Carbon dioxide is transported from the tissues to the lungs through the blood in three major ways:
1. In dissolved state (7%): As $CO_2$ is highly soluble, about 7% of it dissolves directly into the blood plasma and is carried to the lungs.
2. As Carbamino-haemoglobin (20-25%): $CO_2$ binds reversibly to the globin part of haemoglobin in the RBCs. This binding is heavily influenced by the high partial pressure of $CO_2$ at tissue sites.
3. As Bicarbonate ions (70%): This is the major pathway. In the RBCs, the enzyme carbonic anhydrase facilitates the reaction of $CO_2$ with water to form carbonic acid, which dissociates into bicarbonate ions ($HCO_3^-$) and hydrogen ions ($H^+$). These ions travel in the plasma. At the lungs, where $pCO_2$ is low, the enzyme runs the reaction in reverse, releasing $CO_2$ to be exhaled.
Q6. Define Oxygen Dissociation Curve. Can you suggest any reasons for its sigmoidal pattern? Explain the factors that cause the binding and dissociation of oxygen.
Answer: A graphical representation obtained by plotting the percentage saturation of haemoglobin with oxygen against the partial pressure of oxygen ($pO_2$) is called the Oxygen Dissociation Curve. It has a sigmoidal (S-shaped) pattern because the binding of the first oxygen molecule to haemoglobin increases its affinity to bind subsequent oxygen molecules, leading to a steep rise in saturation, which eventually plateaus as all sites fill up.
Factors favoring binding (at Alveoli): High $pO_2$, low $pCO_2$, low $H^+$ concentration, and lower temperature.
Factors favoring dissociation (at Tissues): Low $pO_2$, high $pCO_2$, high $H^+$ concentration, and higher temperature. These conditions prompt haemoglobin to release its bound oxygen to the needy tissues.
Case-Based / Competency-Based Question (4 Marks)
Q7. Read the situation and answer the questions.
A 55-year-old man visits a clinic complaining of severe shortness of breath during minimal physical activity. The doctor observes his breathing and notes that his chest appears permanently somewhat inflated (barrel chest). Upon taking a medical history, the doctor learns the man has smoked two packs of cigarettes a day for 30 years. The doctor suspects a chronic respiratory disorder.
(a) Based on the history, which specific respiratory disorder is the man most likely suffering from?
(b) What exact structural damage occurs in the lungs during this disease?
(c) How does this structural damage affect the physiology of gas exchange?
Answer:
(a) The man is most likely suffering from Emphysema, heavily associated with cigarette smoking.
(b) In emphysema, the delicate alveolar walls are chronically damaged and destroyed.
(c) Because the walls of multiple small alveoli break down to form fewer, larger sacs, the total respiratory surface area available for the diffusion of gases is drastically decreased, causing chronic oxygen starvation during activity.
Assertion-Reason Question
Q8. For the following question, two statements are given—one labeled Assertion (A) and the other labeled Reason (R). Select the correct answer.
(a) Both A and R are true, and R is the correct explanation of A.
(b) Both A and R are true, but R is not the correct explanation of A.
(c) A is true, but R is false.
(d) A is false, but R is true.
Assertion (A): The regulation of respiratory rhythm is primarily dependent on the changing levels of oxygen in the blood.
Reason (R): A chemosensitive area adjacent to the rhythm centre is highly sensitive to changes in $CO_2$ and hydrogen ions.
Answer: (d). The assertion is completely false. The role of oxygen in regulating respiratory rhythm is quite insignificant. The reason is a true statement; the chemosensitive area is indeed highly sensitive to $CO_2$ and $H^+$, which are the true chemical drivers of our breathing rate.
End of Notes.
Students, make sure you understand the difference between lung volumes and capacities, and memorize the factors affecting the oxygen dissociation curve. They are favorite topics for board exams. Happy studying!
Read Also:
Class-11 Physics All Chapters
For official syllabus and textbooks, visit the
NCERT Official Website.